It is probably an understatement to say that life with juniors during the residency training is a milestone in the profession. This past few months has been a period of adjustment for us, “senior” residents in the Internal Medicine Department. As a starting department, birthing pains are common and definitely expected. It is still, however, a headache...a load of headache.
These past few months have been terrible for me. It even lead me to doubt my compassion, competency and knowledge in the field. Certainly, I'm no expert, far from it. However, this feeling of inadequacy is stifling and suffocating. I do believe that this is not my own doing but rather of external forces. It may be because of undue expectations from me by my juniors or their superfluous idealism misplaced at the very least. Or worse, their self-inflated egos may have reached critical levels. I know this type of person. I have seen them in medical school and I always avoided this type of toxicity. Excellence does not need to trample other people.
My analysis, the junior may be too competitive and feels like I'm a target or an anchor for his competitive drive. Lord, have mercy! I'm in a point in my life where tranquility and learning is more important than the appearance of expertise. My competitive drive and compass is anchor on myself growing and learning. Can't he/she/it just compete with itself?
I realized I have to beat him/her/it with his game. And hopefully, the positive thing that will come out of it, is a worthy opponent.
It's a good thing we have this outlet called writing...er...blogging.
During our usual critical appraisal and research updates, I had a light bulb moment. I was thinking about Pubmed and how it provided me with a lot of access to journals and information. It definitely helped me grow in my journey as a resident and physician.
I asked myself, if Pubmed and Pubmed Central are the same entities. Of all the things I have to think about. I had to ruminate on this.
I've always thought that Pubmed and Pubmed Central was synonymous. I didn't even bother to research or was even curious until today. I just thought that Central was just the last name of Pubmed.
Briefly, Pubmed is a free resource supporting the search and retrieval of biomedical and life sciences literature with the aim of improving health–both globally and personally. It was developed and is maintained by the National Center for Biotechnology Information (NCBI), at the U.S. National Library of Medicine (NLM), located at the National Institutes of Health (NIH).
Pubmed Central (PMC) on the other hand, is a free full-text archive of biomedical and life sciences journal literature at the U.S. National Institutes of Health's National Library of Medicine (NIH/NLM). It serves as a digital counterpart to the NLM extensive print journal collection; it is a repository for journal literature deposited by participating publishers, as well as for author manuscripts that have been submitted in compliance with the NIH Public Access Policy and similar policies of other research funding agencies
Sounds the same to me.
Upon further digging, I was able to find some resource that really states they are two different systems although maintained by the same institution.
Bottom line, PubMed citations come from 1) MEDLINE indexed journals, 2) journals/manuscripts deposited in PMC, and 3) NCBI Bookshelf. Which means PubMed has a greater scope for researching articles.
I think the lesson here for me is that sometimes, what we take for granted as systems in place are themselves worth investigating.
While researching on Diabetes and deaths related with it, I stumbled upon an updated resource on mortality in the Philippines. Great information worth sharing.
According to the Philippine Statistics Authority, the reported deaths in 2019 reached 620,414. This is an increase of 5.0 percent from the 590,709 registered deaths in 2018. This is equivalent to a crude death rate of 5.8, or about six (6) deaths per thousand population in 2019. This corresponds to an average of 1,700 deaths per day, which translates to 71 deaths per hour or one (1) death per minute in 2019. This report was released last January 5, 2021.
How does the Philippine Statistics Authority (PSA) obtain the data for processing?
Data on deaths presented in this release were obtained from the Certificates of Death (Municipal Form No. 103) that were registered at the Office of the City/Municipal Civil Registrars all throughout the country and forwarded to the Philippine Statistics Authority. Information presented includes registered deaths which occurred from January to December 2019. Cumulative figures for 2019 reflect updated data which excludes fetal deaths present in the processing of regular deaths and may differ from preliminary counts previously published. Fetal deaths as well as deaths of Filipinos that occurred abroad which were reported to the Philippine Foreign Service Posts are presented in a separate report.
What are the top 10 causes of deaths in the Philippines?
The above figure shows the ten leading causes of death in 2019. Among the total deaths, ischaemic heart diseases were the leading causes of death with 97,475 or 15.7 percent of the total registered deaths. Neoplasms, commonly known as “cancer”, were the second leading causes of death with 68,657 (11.1%), followed by cerebrovascular diseases also commonly known strokes with 63,548 (10.2%).
Some thoughts though, I assume that deaths due to myocardial infarction are clumped or group in the ischaemic heart diseases. Not all diagnosed ischaemic (ischemic) heart disease die upon diagnosis although this is a serious medical condition. It would also be interesting to find out the different cancers that make up the deaths under the neoplasm category. I also would like to know what conditions are classified under the chronic lower respiratory tract infections. Lastly, the classification of “other heart diseases” is also confusing. Maybe they also clamp together all other heart diseases not under ischemic heart disease. What could be the top 1 disease under the other heart diseases? Is it congenital heart disease or maybe cardiomyopathy or even pericarditis or maybe even something else?
How about the deaths for 2020?
We will probably know more later this year or early next year.
A moment of relief was felt yesterday. It would mark the end of my presenting, at least for a while until my next one. I've been presenting since December 2020 for my grand rounds presentation and my inter-hospital presentation. I was supposed to present the census for the months of October and November 2020 but this was further moved to January 2021. Due to work-related scheduling problems, my presentation was further split into two parts, the census for the previous months and a presentation on the mortality report. It was very taxing but nevertheless it afforded me more time to prepare my presentation.
What a welcomed relief! This one is for the books … just another chapter in the chronicles of residency.
Ascites is a common complication of chronic liver diseases and is related to the extent of portal hypertension.
Paracentesis is a procedure in which a needle or catheter is inserted into the peritoneal cavity to obtain ascitic fluid for diagnostic or therapeutic purposes. Ascitic fluid may be used to help determine the etiology of ascites, as well as to evaluate for infection or presence of cancer.
I had little knowledge of the procedure prior to my residency. During my internship days at the Zamboanga City Medical Center, I was not able to observe the said procedure. I only have the faintest academic idea of what it was and its purpose.
Thankfully, the through the patience and dedication of my consultant, I was able to do the procedure through his proper guidance. I also had to read up on the procedure to familiar myself with the procedure. There are a lot of literature available in the internet to gain proper knowledge, however since paracentesis is a skill we also need experiential knowledge.
As a resident I learned about the purpose of SAAG. The serum-ascites albumin gradient or gap is a calculation used in medicine to help determine the cause of ascites. A simple calculation that can help determine what caused the ascites, subtracting the albumin concentration of ascitic fluid from the albumin concentration of serum obtained on the same day.
Below is the algorithm that I came across in my readings.
A SAAG of >1.1 g/dL is 97% accurate in detecting portal hypertension.
In the future, I should order the serum albumin at almost the same time the procedure is done. Moreover, I should be able to order the materials needed for the procedure more efficiently without consulting the ever trusty IM platinum often.
The procedure may be the first of many in my residency training and I should develop the habit and the skill in doing this simple yet important procedure for my future patients.
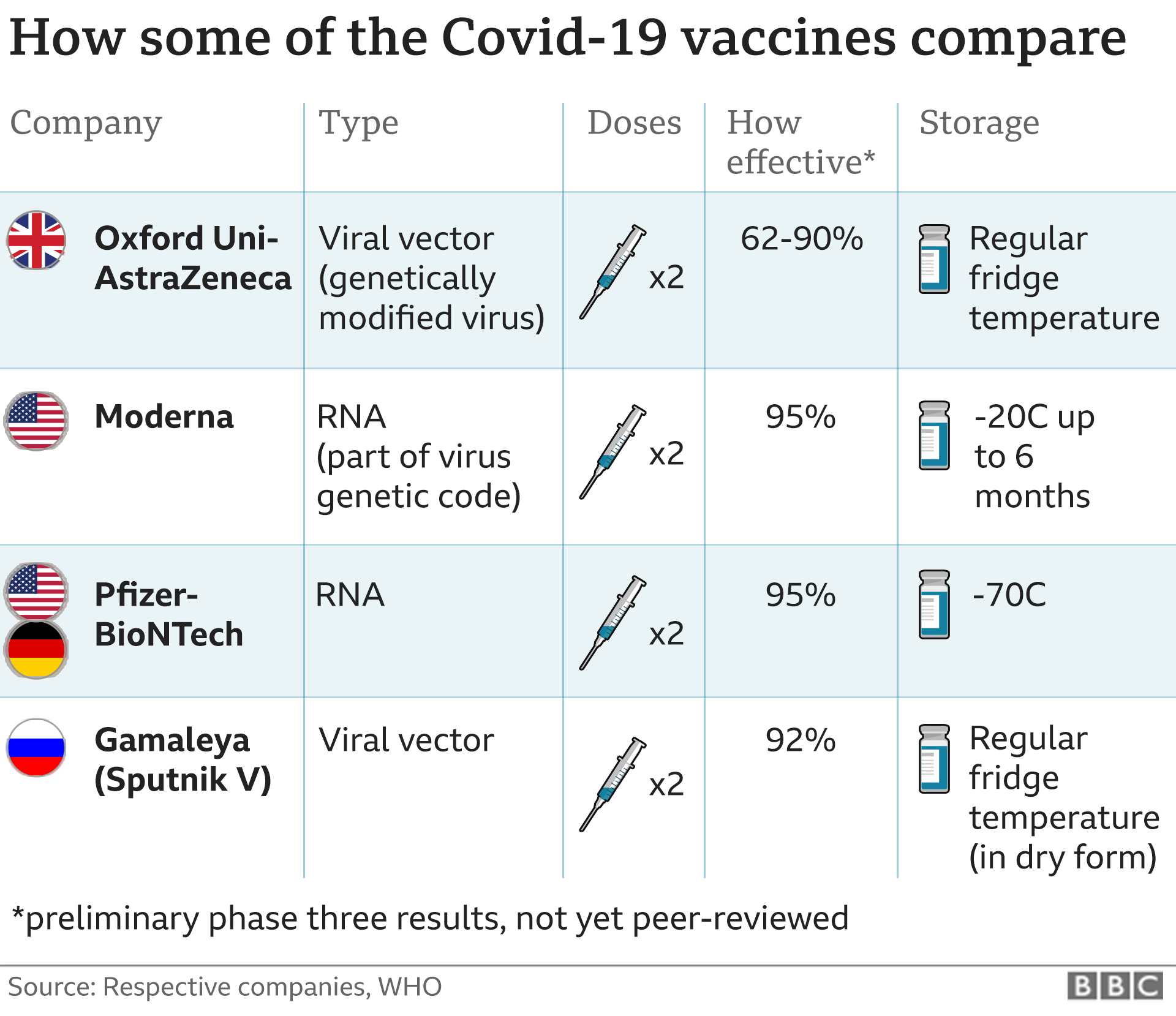
I'm not going to pretend that I understand the complexities of molecular bioengineering. But here's a great summary that delivers great information on the vaccine.
Imagine you are a healthcare worker. Imagine further that we are in a pandemic.
What mindset should he or she have?
Wouldn't it or shouldn't it be the interest of all, the interest of the most?
I'd like to discuss on two commonly used principles in medical ethics. The principle of Beneficence and Non-Maleficence. All healthcare providers must strive to improve their patient’s health and avoid in every situation causing harm to their patients. In basic terms, it means to do good and do no harm. Simple to say but never easy to execute in health care because there can be gray areas.
Today, I learned that a medical practitioner who reported for duty, for work, not feeling too good and under the weather, was tested positive for SARS-COV2. Certainly, I can commiserate with his/her predicament. No one wants to be tested positive. There is not one health worker who wants to be positive.
And then, there's the rub.
A medical practitioner, deemed a front-liner, deemed the most knowledgeable and expert in the science of the transmission and infectiousness of SARS-COV2 decided to go to work. In doing so, inevitably exposing other members of the healthcare team and will be compounded when each member goes home to their family and love ones.
The end.
Some key lessons learned:
1. Protect yourself always. When you let your guard down, that's the time when you will be reminded of Murphy's law.
2. Trust no one. Even your family, loved ones and friends. It is your inner circle that has the highest probability of infecting you more than a random stranger in a grocery store.
3. Worrying over being infected is stressful.
Day 2 of the 50th Philippine College of Physicians Virtual Annual Convention.
Today, I learned about the Declaration of Geneva. No, the declaration and the Geneva Conventions are not the same. The former document is not about the humane treatment of prisoners of war and the humanitarian conduct during armed conflicts. This is another document and it is a modern form of the Hippocratic Oath. The Declaration of Geneva is one of the World Medical Association’s (WMA) oldest policies adopted by the 2nd General Assembly in Geneva in 1947. Currently, it is on its 7th version and was amended last 2017.
There was a line that was purposely pointed out during the PCP Annual Convention. It states:
“I WILL ATTEND TO my own health, well-being, and abilities in order to provide care of the highest standard;”
People tend to forget that health practitioners and medical professionals are people that can get tired and stressed out. But what I realized more is that, it is also incumbent upon the health care worker to attend to his personal needs. This exact line was also missing from the previous iterations of the document. It most probably reflects on the attitude of the health professionals as well.
Don't quit. Rest if we must. For if we are in our best state, we are able to help treat and/or cure the patient.
Do you want to read the complete WMA Declaration of Geneva? You can find it here.
A little over a year ago, while I was doing my usual rounds in the hospital, a surgical consultant approached me and asked why I was wearing a facemask while I was in the ward. He even remarked that I looked silly and that instead I looked like I was harboring a respiratory infection with my facemask on.
I smiled and answered, I wear these masks so that I protect myself and my patients from the possibility of respiratory infections. He laughed rather heartily. Like I was such a joke.
I remember this incident because I saw him a few days ago. He was with his facemask and heavy duty faceshield. I'm sure he does not recall me or that conversation with him. This time, I thought to myself, “Where is your machismo now? I thought we don't have to protect ourselves from possible infections.”
How can a consultant (boss) bully a resident in training?
There are probably a number of ways to bully a resident in training. But I think the brilliant once disguised themselves in “learning atmospheres”. Ahh, yes, the ones were you (the resident) is asked to present a case with less than 24 hours to prepare. It makes you feel that the objective really is to deprive you of valuable resource – sleeping time. Time that is scarce in the profession of medicine. She was probably having her bad hair days.
If the objective is truly a learning experience, then ample preparation should be given to the learner.
But what can a resident do, but to shut up and do or comply with what she asked. This way the problem goes away and hopefully her mood improves. Every resident must cope up and survive. Hoping for better days then...
P.S.
I was able to comply with her “request”. But I just need to vent for sanity's sake.