Closing Remarks for 1st episode of Local WISDOM webinar
Entry #45
I delivered the Closing Remarks for the 1st episode of Local W.I.S.D.O.M. or Local Webinars on Innovation and Strategies on Advancing Occupational Medicine of the Philippine College of Occupational Medicine – Zamboanga Peninsula Chapter. The following was the content of the speech.
Good evening, everyone. On behalf of the PCOM Zampen Chapter, we would like to thank everyone for being with us in our first episode of Local WISDOM.
In closing the 1st episode of Local WISDOM or Local Webinars on Innovation and Strategies on Advancing Occupational Medicine, we are reminded that occupational medicine plays a crucial role in ensuring the health and well being of workers in diverse industries.

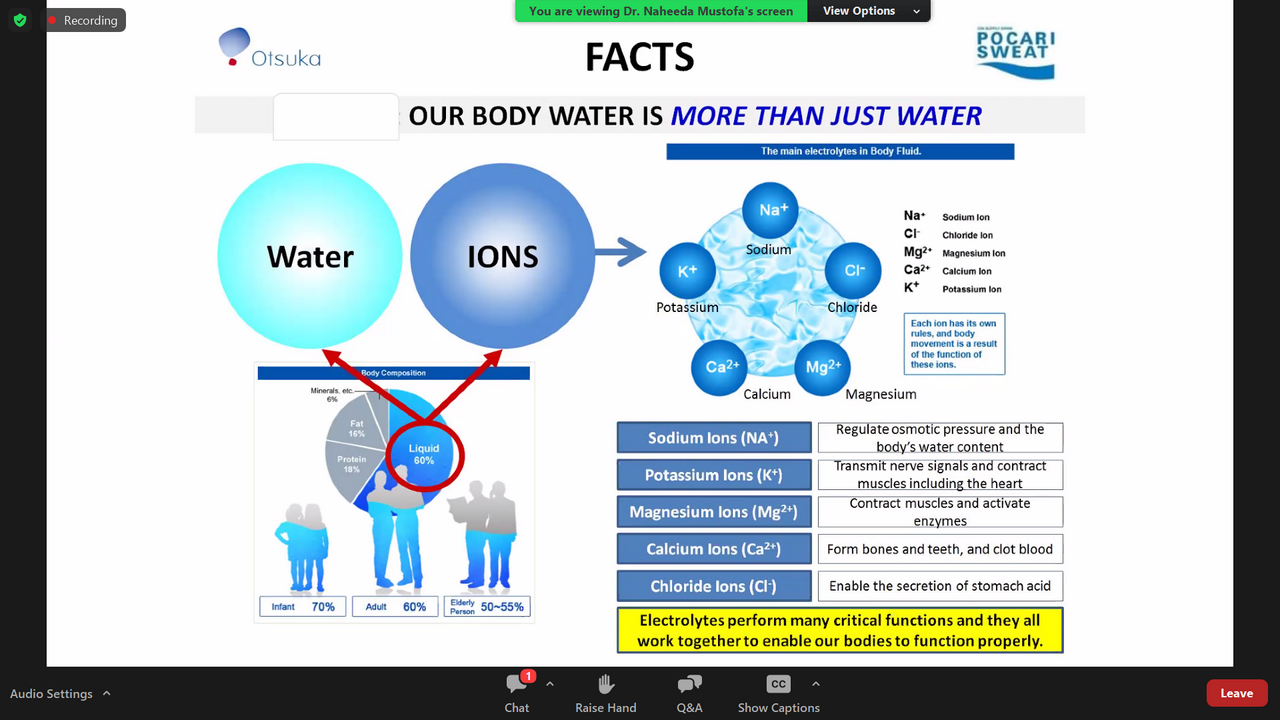
Hydration is important and is often neglected. Our body water is not just made up of water. Electrolytes enable our bodies to function properly. Hence, replacement of losses must not only be water alone. Finding the right and proper balance is important, right food and right hydration.
Finally, this project aims to provide accessible, high-quality information on the latest innovations, best practices, and strategic approaches in occupational health and safety. We hope to see you in our next episode. Good evening once again to all the members and guests.






